Knowing the anatomy of the neck will help you prevent neck injuries. You will also be able to quickly detect which muscle, bone or ligament is causing discomfort at the base of your head. So, if you want to learn in depth what this cervical area is, read on.
We will explain the bones, ligaments and muscles in this region of the body and their biomechanics. In addition, you will read about the most common cervical injuries that occur and about the treatments that are currently applied. Don't miss a thing.
Parts and anatomy of the neck
In the anatomy of the human body, the neck plays a vital role. For this reason, we will show you below the main structure that forms the different relationships that this area has in a person:
Bones and joints
The bones that make up the neck are
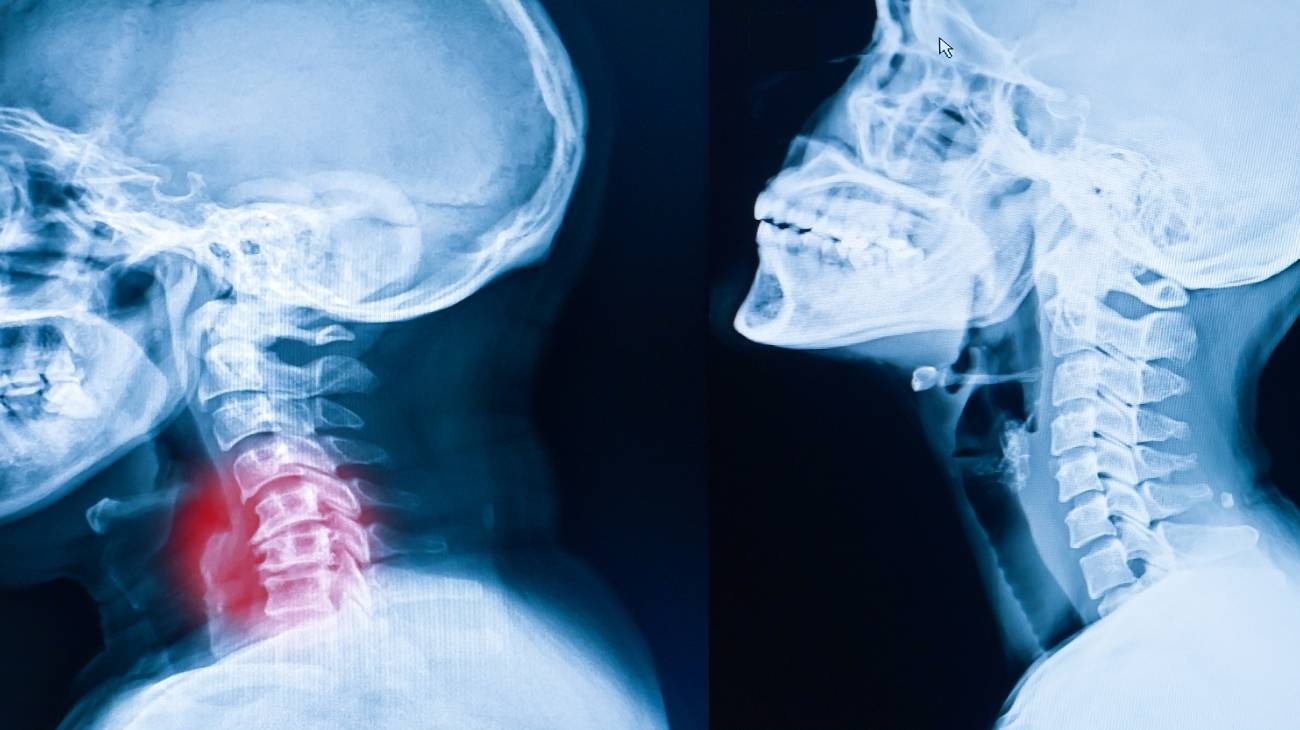
- Cervical vertebrae: Support the cranial cavity, connect the head to the lumbar spine and provide articulatory movements. It is composed of 7 vertebrae, called C1 to C7 inclusive. C1 is also called Atlas and C2, Axis. Within each are the apophyses, tubercles and nerve grooves.
- Hyoid: Its function is to support the tongue and larynx. It has a symmetrical U-shape and is located below the mandible, between the third and fourth vertebrae. It is one of the few odd bones that have no articulation, as it is suspended between ligaments and muscles.
- Sternal shaft: This is the upper part of the sternum, bounded by the jugular notch, the clavicular incisure and the costal part of the first notch. The shaft of the sternum is variable in shape and articulates with the body of the sternum by means of a fibrocartilage disc.
- Clavicle: This bone may be found as an integral part of the shoulder, but is also considered to be part of the skeleton of the neck. It is a flat, elongated bone that joins the manubrium of the sternum to the scapula.
So far we have talked about the bones that make up the neck, but these have to have the capacity to produce movements in the human anatomy, which is why the joints are needed.
See below all the articular parts found in the neck:
- Atlantooccipitals: They are located between the atlas and the apophyses, reaching the foramen magnum. Their main function is extension, lateral tilt (or abduction) and flexion of the head.
- Atlantoaxial: Taking the axis of the axis tooth as its axis, it rotates the atlas to perform head rotation movements. Characteristic is the lack of intervertebral discs between these bones.
- Uncovertebral: These are flat joints located in the unciform processes to give movement to the cervical vertebrae.
- Cygapophyseal: Their main function is to limit movement between two vertebrae, so they need to be located between them.
- Intervertebral: As their name indicates, these fibrocartilaginous discs are located between the cervical vertebrae, which allows a small torsional movement between them.

Muscles
The muscular structure of the neck is made up of the following tissues:
- Stylohyoid: Its function is to support the hyoid bone, which supports the mandible. It arises from the styloid process of the temporal bone in the skull and is located above the posterior belly of the digastric groove.
- Hyoglossus: By means of the hypoglossal nerve, it compresses and retracts the tongue so that it becomes more or less convex. Its origin is the hyoid bone, at the top.
- Mylohyoid: The upper part is located in the mandible, above the anterior belly of the digastric and its course is generated below the geniohyoid muscle. Its work is related to maintaining the hyoid bone, the tongue and the base of the mouth.
- Omohyoid: It is responsible for controlling the activity of the cervical fascia and the hyoid. It arises from the upper part of the scapula and is related to the hypoglossal nerve.
- Scalene: It is divided into anterior, middle and posterior. It is triangular in shape and arises from the cervical vertebrae C3, C4, C5 and C6. Its main function is to rotate the neck and elevate the first and second ribs of the thorax. It is characterised by having a different size according to the development of the muscle performed by the person.
- Sternocleidomastoid: It can be seen externally from the lateral aspect of the neck, as it originates in the manubrium of the sternum and inserts in the mastoid process of the nape of the neck. It is responsible for moving the articular bodies of the skull and cervical vertebrae. It also acts in the extension and elevation of the head and chin and also of the shoulder.
- Splenius: This muscle, also known as splenius, arises from the ligament located at the nape of the neck and runs towards the base of the skull. Its mission is to rotate and tilt the head to the same side, although it is also capable of extending the neck and skull.
- Elevator of the thyroid: it is responsible for raising the isthmus of the thyroid towards the hyoid bone. The reason for this is currently not known with certainty.
- Angular of the scapula: This muscle is responsible for controlling the movements of the scapula, in its elevation and adduction, which is why it is also known as the levator scapulae. It arises from the transverse processes of the cervical vertebrae C1 to C4 and inserts on the medial border of the scapula.
- Thyrohyoid: This is one of the shortest muscles in the anatomy of the neck, as it inserts into the sternohyoid, arising - in an oblique line - from the thyroid cartilage. The mission of this tissue is to lower the hyoid or to raise the larynx if it is in contraction.
- Sternothyroid: Its origin is in the manubrium of the sternum and in the first rib and it inserts into the thyroid cartilage, in an oblique line. It also works to lower the larynx so that the larynx does the same for the hyoid.
- Cricothyroid: In charge of stretching and tensing the vocal cords, its origin is in the cartilage of the larynx - called the cricoid - and the thyroid cartilage.
- Arytenoepiglottis: The epiglottis works to prevent food from entering the trachea through this muscle. It is located between the larynx, the arytenoid cartilage and above the cartilaginous structure of the epiglottis.
- Transverse arytenoid: This is the muscle responsible for regulating the laryngeal lumen through the glottis. It is therefore a single muscle found in the posterior part of the larynx and in the arytenoid cartilages.
- Pharyngoglossus: This muscle works as a constrictor of the pharynx at the top. It also directs the movements of the tongue.
- Geniohyoid: Also known as geniohyoid, it is responsible for widening the pharynx, acting as a depressor of the floor of the mouth by immobilising the muscles of the hyoid bone and pushing on the hyoid bone. The lower spine of the chin sees its origin at the hyoid bone.
- Genioglossus: Its action is to move the tongue in the mouth, to pull it out and to push it in. It arises from the chin of the mandible and inserts into the upper part of the tongue and the hyoid bone.
- Superior lingual: It arises from the tongue and inserts on the hyoid and glossoepiglottic. Its function is to retract and raise the tip of the tongue.
- Longus capitis: This muscle is located between the transverse process of the C3 to C6 vertebrae and inserts into the occipital bone, and its function is to flex the neck.
- Oblique: It is divided into two sections, the greater and the lesser. From the axis process it inserts into the transverse process of the atlas vertebra and into the occipital bone to turn the head.
- Rectus: This muscle is responsible for flexing the head and neck. It arises between the C1 and C2 vertebrae (precisely in the transverse process of the atlas) and inserts into the occipital bone. It can be divided into anterior and lateral rectus.
- Posterior rectus: Unlike the anterior muscle, this tissue arises from the spinous process of the axis and inserts into the occipital bone in a nuchal line. The work it performs is also that of extending and rotating the neck. It can be divided into posterior major and posterior rectus minor, which arises from the tubercle of the posterior arch of the atlas.
- Digastric: It arises from the mandible and the mastoid process of the temporal bone and inserts, among other places, in the hyoid bone. The work it performs in the anatomy is to carry forward and backward the mandible and to elevate the hyoid.

Ligaments
The ligaments located in the neck are:
- Anterior longitudinal: It is characterised by being continuous and joins the base of the cranial cavity, running along the entire spinal column until it reaches the surface of the sacrum. It is characterised by regulating the extension of the cervical spine to prevent inappropriate elongation of the neck.
- Posterior longitudinal: Unlike the ligament mentioned above, this band is not very elastic and is wider and thicker. It is responsible for preventing hyperflexion of the neck; in other words, it ensures that head movements are not abrupt and exceed the limits when the skull moves forward.
- Intertransverse: These are discontinuous ligaments that are responsible for joining the transverse processes of the vertebrae with the muscles and bones.
- Interspinous: These are also discontinuous and are formed from the spinous processes with the posterior supraspinous ligament and the anterior yellow ligament.
- Supraspinous: Extends from one spinous process to another to hold the cervical structure in the correct position. On the other hand, it joins the skull to the process of the C7 vertebra and to the tubercle of C1.
- Yellow: This class of fibrocartilages are considered discontinuous ligaments and are found between the spinal canal with the upper vertebra. Their mission is to help the extension and separation of the cervical vertebrae at the moment of flexion.
- Transversus atlas: The job of this ligament is to prevent the odontoid process from moving backwards so that the rotation of the head can perform the pivoting movement correctly.
- Nuchal: It arises from the spinous process of the C1 vertebra and extends to the first thoracic vertebra to prevent anterior flexion of the neck. It also attaches some muscles to this skeletal structure.
- Atlantooccipital and atlantoaxial: These two ligaments join the arches of the atlas and axis to the external part of the foramen magnum.
- Pharyngoepiglottic: This ligament is responsible for joining the epiglottis to the upper part of the pharynx.
- Glossoepiglottic: joins the glottis to the tongue.
- Thyroepiglottic: this is responsible for joining the thyroid cartilage to the epiglottis.
- Thyrohyoid: It runs from the hyoid bone to the thyroid cartilage. It is related to the medial and lateral thyrohyoid ligaments which attach to the thyroid on both sides.
- Vocal: Also known as the inferior thyroarytenoid ligament, it is responsible for covering the vocal cords and attaching them to the larynx.
- Vestibular: It is located in the vocal fold. It is also called Ventricular. Its mission is to join the thyroid to the arytenoid cartilage.
- Sesamoid: A set of small ligaments located on the lateral side of the arytenoid cartilage and the corniculate cartilages.
- Hyoepiglottic: connects the hyoid bone to the glottis.
- Cricothyroid: This is the ligament responsible for working with the cricothyroid joints.
- Cricoarytenoid: The cricoarytenoid joints maintain their position thanks to the work of this ligament.

Best products for neck and shoulder pain relief
Bestseller
-

Acupressure Mat and Pillow (Black/Gray)
$49.95 -
Acupressure Mat and Pillow (Green/Navy)
$49.95 -
Acupressure Mat and Pillow (Pink/Bordeaux)
$49.95 -
Acupressure Pillow (Black/Gray)
$29.46 -
Acupressure Pillow (Green/Navy)
$29.46 -
Acupressure Pillow (Pink/Bordeaux)
$29.46 -
Electric Muscle Massager Gun
$177.03 -
Electric Neck & Shoulders Massager
$35.36 -

Ice Massage Roller Ball (Black)
$39.95 -
Ice Massage Roller Ball (Green)
$39.95 -
Ice Massage Roller Ball (Pink)
$39.95 -
Microwave Heating Pad for Neck & Shoulder Pain Relief (Hearts)
$24.95 -
Microwave Heating Pad for Neck & Shoulder Pain Relief (Oxford)
$24.95 -
Microwave Heating Pad for Neck & Shoulder Pain Relief (Sport)
$24.95 -
Microwave Heating Pad for Neck Pain Relief (Hearts)
$19.95 -
Microwave Heating Pad for Neck Pain Relief (Oxford)
$19.95 -
Microwave Heating Pad for Neck Pain Relief (Sport)
$19.95 -
Microwaveable Heating Pad for Pain Relief (Hearts)
$19.95 -
Microwaveable Heating Pad for Pain Relief (Oxford)
$19.95 -
Microwaveable Heating Pad for Pain Relief (Sport)
$19.95 -
Mini Electric Massager Gun
$58.97 -
Pack 2 Peanut Massage Rollers
$19.95 -
Reusable Ice Pack for Neck & Shoulders Injuries
$24.95 -
Shoulder Support Brace (Black)
$24.95 -
Shoulder Support Brace (Green)
$24.95 -
Shoulder Support Brace (Pink)
$24.95 -
Trigger Point Massage Stick (Black)
$14.95 -
Trigger Point Massage Stick (Green)
$14.95 -
Trigger Point Massage Stick (Pink)
$14.95 -
Vibrating Foam Roller
$35.36
































Biomechanics of the neck and spinal column
The activity of the neck and spine can be studied by means of biomechanics, which is a discipline that analyses the phenomena that occur in this part of the body after applying different types of natural forces. So, if you want to know the energetic performance of a person's organism, it is necessary to know the types of biomechanical movements in this area.
We show you below the actions that the neck can perform
- Flexion: This is produced when the chin touches the thorax, modifying the angle of the neck by 90 degrees towards the front of the body. It is produced by the sliding of the upper vertebrae over the lower vertebrae.
- Extension: This is the opposite movement to flexion, placing the neck in its natural position. In this case, the gelatinous substances of the discs move backwards to provoke the movement. The sternocleidomastoid muscles work together with the deep muscles of the back.
- Lateral tilt: This is also referred to as lateral flexion, which occurs when the pinna rests on the shoulder. The axis of the neck rotates 45° due to the contraction and flexion of the head muscles.
- Rotation: Thanks to the articulatory body of the atlas and axis (C1 and C2) it is possible to rotate the head 90° to the left and right, causing an alignment between the shoulder and the chin.
It is also useful to analyse the biomechanical movements of the spine, which are:
- Flexion: The amplitude generated by the vertebral body is 30° and is obtained by moving the shoulders and head forward, causing the intervertebral discs to increase in thickness in the posterior area.
- Extension: This movement tilts the overlying vertebra backwards, causing the anterior part of the disc to increase in thickness. In this way it is possible to achieve an amplitude of 40 degrees in relation to the spinal axis.
- Lateral tilt: The tilt generated is between 20° and 30° thanks to the work done by the overlying vertebrae and the discs bending to the concave and convex side, respectively.
- Rotation: It is possible to achieve rotation only in the cervical and dorsal part while in the lumbar spine its range does not exceed 2°, but if one considers the whole spine movement, in total the rotation is 10°.
Most common neck injuries
As the neck is one of the most complex structures due to the large number of muscles, bones and ligaments found in the area, it is possible for this area to be injured by a variety of factors.
Therefore, we will show you below what are the most common neck contusions, take a look.
Types of neck injuries
See what are the most common types of neck injuries people suffer from:
- Cervical muscle contractures in the neck: Contractures are involuntary tensions that occur in the muscles due to the accumulation of metabolites in the fibres because the blood cannot eliminate them when exchanging oxygen and nutrients. They are usually caused by sudden movements and strenuous activity.
- Cervical sprain in the neck: When a micro-break or tear occurs in the fibres of the ligaments that join the different vertebrae it is known as a neck or cervical sprain. This can be caused by bad posture, lack of exercise and an incorrect diet, among other factors.
- Cervical osteoarthritis in the neck: Osteoarthritis is caused by a variety of factors, the most common being the body's own autoimmune system, age and the daily activities the patient performs. It is a disease that causes pain, inflammation, stiffness and wear and tear on bones and cartilage. There is no cure.
Sports neck injuries
Learn about the common neck injuries that sportsmen and women suffer as a result of these activities:
- Sports injuries of the neck in football: Among the most common injuries that occur in this activity are contractures of the sternocleidomastoid, scalene and angular of the scapula. There are also injuries to the oblique and rectus, causing stiffness in head movements. On the other hand, fractures and trauma to the clavicles are the most common.
- Sports injuries to the neck, head and face in boxing: The injuries suffered in this sport can be varied. Jaw and neck injuries occur slightly more than 10% of the time when a person visits a doctor's office. Contractures suffered in the long head, oblique, rectus, sternocleidomastoid, scalene and splenic muscles are the most common tissue strains.
- Neck injuries in Yoga: Although it is not an extreme sport, people who practice this discipline suffer from different neck injuries. Among the most common are muscle stiffness caused in the trapezius, oblique, suboccipital and sternocleidomastoid muscles. Fractures are not common in this type of practice.
Diseases and ailments in the neck

Ailments in the neck can be caused by various diseases, which are discussed below:
Meningitis
Inflammation of the meninx causes pain in the brain and the base of the skull. This is due to the fact that the spinal cord does not function properly and the infection and the signs gradually increase if not treated urgently.
Cancer
Some oncological diseases can cause constant pain in the neck. This can have different causes due to a lack of platelets and blood cells in the body caused by the cancer cells themselves.
Herniated discs
These alterations in the intervertebral discs (and also osteophytes or bone spurs) cause pinching of the nerve roots located in the neck. This causes pain and joint stiffness due to the limited space for the nervous system to function properly.
Tonsillitis
Inflammation in the palatine tonsils promotes pain in the neck due to the large number of autoimmune cells generated by the body to combat the condition, resulting in discomfort at the base of the cranial cavity.
Osteomyelitis
The bone marrow can usually suffer from an infection caused by bacteria or fungi. This causes swelling and pain in the neck due to the proximity of the bone marrow to the nerves in this part of the body.
Diabetes
People suffering from this metabolic disease with high blood glucose levels are more prone to neck pain. Although the reason for this relationship is not yet established, recent studies have shown this connection in a large number of patients.
How can we relieve neck pain through complementary and non-invasive therapies?
It is possible to relieve neck pain through therapies that can be used in a complementary and non-invasive way. See below which ones are currently the most commonly used:
Heat and cold therapy
This type of treatment consists of applying heat in the same session, then continuing with cold and finishing with the first temperature. Care must be taken, as the application should not exceed 20 minutes in total.
- The heat causes the vessels of the capillary walls to dilate causing a greater blood supply to the affected area, the use of microwave heat packs is recommended.
- While cold acts as an analgesic agent. It is possible to apply this therapy by means of ice gel packs.
Compression therapy
By means of special collars and splints it is feasible to immobilise the neck so that the muscles, ligaments and joints return to their normal position. This will cause the area to deflate more quickly, increase the blood supply and reduce pain. In some cases, the use of sports compression shoulder braces may be recommended to support a larger area of the body.
Massage therapy
This is one of the most commonly applied therapies in this type of ailment due to the direct rubbing of the muscles and tendons in the affected area. In this way the physiotherapist provokes internal heat, thus stimulating the blood flow to reduce inflammation and pain in the patient. This treatment also aims at complete relaxation of the person, which is why self-massage is a good idea. Electronic massagers are suitable for this purpose.
Acupressure therapy
Acupressure consists of pressing certain parts of the patient's body with the fingers and palms, without using any external elements. It is important to bear in mind that it does not only work on the neck but on the whole human anatomy. The aim of this therapy is for the patient to find mental harmony in order to reduce muscular contractions in a natural way.
Thermotherapy
Although we have already talked about the benefits of heat as a dilating agent of the capillary walls, it is important to clarify at this point that this therapy uses only heat to obtain these effects (unlike cold and heat treatment). Thermotherapy can be applied by means of different techniques, the most common being the use of microwavable thermal pillows and hot water baths.
Cryotherapy
Care must be taken with the application of cold, either by means of cold pads or ice gel packs, because the effect that cryotherapy can generate may be contraindicated for neck pain. In other words, the use of this therapy must be recommended by the doctor and is only possible when the injury has not exceeded 48 hours.
Electrical muscle stimulation (EMS)
Muscle electrostimulation, or EMS, is a therapy that consists of stimulating muscle contractions through the use of electricity, so as to achieve an effect of activity and hypertrophy as in the gym, but without the need to go to any sports center. This means that you can put your muscles to work without leaving home.
Electrotherapy
This is a technique that seeks relief from pain and some physical ailments through the application of electrical and electromagnetic energy, among other variants, through the skin with the use of conductive pads called electrodes. It is a very safe type of therapy and must be applied by a physical therapist specialized in the manipulation of electricity to treat some kinds of ailments.
Myofascial release therapy
Also known as myofascial induction, this therapy consists of the application of manual massage to treat the shortening and tension generated in the myofascial tissue that connects the muscles to the bones and nerves. For this purpose, various massage techniques are used that focus on the so-called trigger points.
Percussion Massage Therapy
Vibration or percussion massages are precise, rhythmic and energetic strokes on the body to achieve relief from some annoying symptoms when muscle fibers are tightened, often by a high workload on them and that has left trigger points in the muscle fibers.
R.I.C.E Therapy
The R.I.C.E. therapy is the first and simplest of the treatment protocols for minor injuries. It appears in the sports field to deal with accidents involving acute injuries. For many years, it has been considered the most suitable for its speed and results.
Trigger points therapy
Myofascial pain points or trigger points are knots that are created in the deeper muscle tissues, causing intense pain. The pain does not always manifest itself right in the area where the point develops, but rather this pain is referred to nearby areas that seemingly do not appear to be related. In fact, it is estimated that more than 80% of the pain they cause manifests in other parts of the body.
Other effective alternative therapies
There are other types of treatments, in addition to those mentioned above, that can be implemented to reduce neck pain.
These are:
- Natural remedies using plants: There are different plants in nature that have healing properties and can be used in the treatment of this condition. Among the most commonly used herbs are ginger, mint, linden, chamomile and rosemary.
- Acupuncture: If what is sought is a mental balance to obtain a general wellbeing of the patient, this therapy can be implemented by means of needles that are placed in different strategic areas of the body.
- Kinesiotherapy: By means of biomechanics and other physiological movements it is possible to stimulate the nervous system. Due to the application of this therapy it is possible to know the correct postures of the neck.
- Aromatherapy: This technique is used to reduce stress in the patient by means of smells that are provoked by direct application or by spraying devices. Citrus fruits, ginger and mint are the most commonly used scents.
- Osteopathy: This alternative therapy seeks to stretch the muscles and ligaments of the neck to return them to their natural position (as well as the bones). Keep in mind that the choice of this therapy must be approved by the doctor to avoid future complications.
References
- Hiatt, J. L. (2020). Textbook of head and neck anatomy. Jones & Bartlett Publishers. https://books.google.es/books?hl=en&lr=&id=42HdDwAAQBAJ
- Norton, N. S. (2016). Netter's head and neck anatomy for dentistry e-book. Elsevier Health Sciences. https://books.google.es/books?hl=en&lr=&id=J9sqDQAAQBAJ
- Kohan, E. J., & Wirth, G. A. (2014). Anatomy of the neck. Clinics in plastic surgery, 41(1), 1-6. https://www.plasticsurgery.theclinics.com/article/S0094-1298(13)00103-X/fulltext
- McIntosh, A. S., & McCrory, P. (2005). Preventing head and neck injury. British Journal of Sports Medicine, 39(6), 314-318. https://bjsm.bmj.com/content/39/6/314.short
- Tysvaer, A. T. (1992). Head and neck injuries in soccer. Sports Medicine, 14(3), 200-213. https://link.springer.com/article/10.2165/00007256-199214030-00006
- Mayou, R., & Bryant, B. (1996). Outcome of ‘whiplash’neck injury. Injury, 27(9), 617-623. https://www.sciencedirect.com/science/article/abs/pii/S0020138396001143
- Mayou, R., & Bryant, B. (2002). Psychiatry of whiplash neck injury. The British Journal of Psychiatry, 180(5), 441-448. https://www.cambridge.org/core/journals/the-british-journal-of-psychiatry/article/psychiatry-of-whiplash-neck-injury/0734BAAAF64DF6C3974E47CCD71203F6
- Gay, J. R., & Abbott, K. H. (1953). Common whiplash injuries of the neck. Journal of the American Medical Association, 152(18), 1698-1704. https://jamanetwork.com/journals/jama/article-abstract/287760
- Hoy, D., Protani, M., De, R., & Buchbinder, R. (2010). The epidemiology of neck pain. Best practice & research Clinical rheumatology, 24(6), 783-792. https://www.sciencedirect.com/science/article/abs/pii/S1521694211000246
- Bovim, G., Schrader, H., & Sand, T. (1994). Neck pain in the general population. Spine, 19(12), 1307-1309. https://europepmc.org/article/med/8066508