- What is a hip fracture and how is it diagnosed?
- What are the types of hip fractures?
- Best products for hip fractures
- What are the causes and risk factors for hip fractures?
- First aid care to treat a hip fracture
- Most indicated treatments for hip fractures
- Rehabilitation after a hip fracture
- Preventive methods to avoid broken hip bones
Over the years, humans tend to suffer from certain diseases that are common in older people. One of these is osteoporosis, which causes the bones to weaken and this, as well as affecting balance, can lead to various injuries such as bone fractures.
Thus, one of the most serious fractures of all is the hip fracture. Given that the hip is a large joint and its breakage implies a pathology that requires the greatest possible attention. For this reason, we would like to highlight what this kind of trauma consists of and what its types, causes, treatments, care methods, etc. are.
What is a hip fracture and how is it diagnosed?
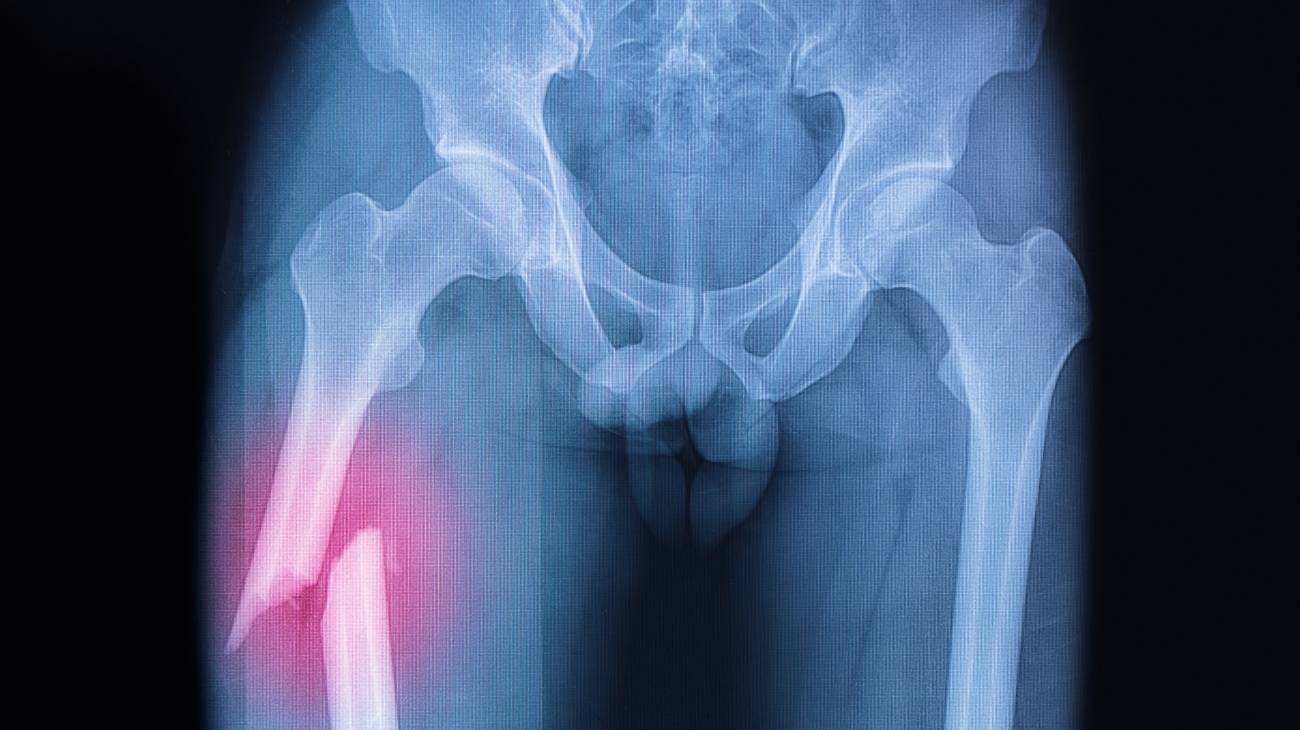
A hip fracture is defined as a break or tear that develops in the proximal extremity of the femur or thigh bone of the joint. Since this is a large joint where the femur meets the pelvis, the head of the femur is inserted into the joint from a cavity formed by the bone known as the "acetabulum". Consequently, once the injury occurs, of course, the femoral head is impacted.
As a result, this type of fracture triggers a serious and particular symptomatological picture consisting of:
- Acute pain in the hip or groin.
- Swelling in the hip area and adjacent areas.
- Bruising at the site of impact.
- Inability to walk or get up from a chair.
- Difficulty bearing weight on the leg on the side of the injured hip.
- Reduced mobility in the injured limb.
- Shortening in size and an outward turn of the leg on the side of the injured hip.
In that sense, in order to diagnose a hip fracture accurately and concisely, in addition to taking into account the main symptoms, the medical specialist must carry out a physical examination of the condition.
Taking into account that a person with this condition has signs such as:
- Inability to stand up.
- Pain on palpation over the proximal femur.
- Inability to lift the affected limb against gravity.
- Shortening and external rotation of the leg.
The specialist doctor will have to carry out a radiological study to examine the abnormal position shown by the hip and leg. In the event that this radiological diagnostic technique does not present the required details to determine a hip fracture and the person continues to show pain or discomfort in the area, it is essential to resort to a magnetic resonance or bone scan in order to look for a fracture in detail.
The doctor will be able to detect where in the long bone that extends from the hip to the knee or femur the tear occurred, either:
- In the neck of the femur, which is the upper part of the femur located below the ball and socket joint or head of the femur.
- In the intertrochanteric region, which is the area just below the actual hip joint. Or, in the part of the upper femur that projects outwards.
What are the types of hip fractures?

Mainly, depending on the location of the fracture at the level of the bone, this type of hip injury is classified as follows:
- Subcapital fracture (Zone 1): Also known as a "femoral neck fracture", this occurs at the level of the femoral neck, between the femoral head and the greater trochanter, mostly below the femoral head. In most cases, they have a propensity to cause damage to the blood supply in this part of the femur.
- Trochanteric fracture (Zone 2): These refer to hip injuries that originate at the level of the trochanter or the area below the neck of the femur. These are also called "transtrochanteric fractures" and correspond to the proximal metaphyseal region of the femur between the two trochanters.
- Subtrochanteric fracture (Zone 3): This is a hip fracture located between the lesser trochanter and a point 5 cm below it. They can affect people of all ages and comprise between 10% and 30% of all hip fractures, approximately.
On the other hand, depending on how it affects the area covered by the joint capsule or is located outside this, other types of hip fracture are distinguished as follows:
- Intracapsular fractures: These usually affect the femoral neck or femoral head (they are associated with hip dislocations and are less common). They consist of injuries that are located on a bone with poorer vascularisation and, therefore, the absence of consolidation or avascular necrosis is frequent. If they are generated in the femoral neck, they reveal other subtypes:
- Type I (incomplete impacted in valgus)
- Type II (complete without displacement)
- Type III (complete with partial displacement)
- Type IV (complete and totally displaced)
- Extracapsular fractures: These are based on those breaks that occur on a bone with good vascularisation and in comparison with intracapsular fractures, these cause greater pain and haemodynamic instability. In addition to this, they handle a subclassification that depends on their degree of stability and basically they are: Stable fractures that have posterior and medial cortical contact once reduced. As well as unstable fractures, which are all the others and those with an inverted line.
Best products for hip fractures
Bestseller
-


Microwave Wheat Bag for Back Pain Relief (Extra Large) (Hearts)
£24,95 -
Microwave Wheat Bag for Back Pain Relief (Extra Large) (Oxford)
£24,95 -
Microwave Wheat Bag for Back Pain Relief (Extra Large) (Sport)
£24,95 -
Microwave Wheat Bag for Neck & Shoulder Pain Relief (Hearts)
£24,95 -
Microwave Wheat Bag for Neck & Shoulder Pain Relief (Oxford)
£24,95 -
Microwave Wheat Bag for Neck & Shoulder Pain Relief (Sport)
£24,95 -
Microwaveable Wheat Bag for Pain Relief (Hearts)
£20,95 -
Microwaveable Wheat Bag for Pain Relief (Oxford)
£20,95 -
Microwaveable Wheat Bag for Pain Relief (Sport)
£20,95 -
Reusable Extra Large Hot & Cold Packs for Back & Legs
£24,95 -
Reusable Gel Ice Packs with Compression Band for Sports Injury
£20,95 -
Wheat Bag for Microwave Classic Bottle Shaped (Hearts)
£20,95 -
Wheat Bag for Microwave Classic Bottle Shaped (Oxford)
£20,95 -
Wheat Bag for Microwave Classic Bottle Shaped (Sport)
£20,95


























-
Back Support Belt (Black)
£39,95 -
Back Support Belt (Green)
£39,95 -
Back Support Belt (Pink)
£39,95 -
Ice Massage Roller Ball (Black)
£34,95 -
Ice Massage Roller Ball (Green)
£34,95 -
Ice Massage Roller Ball (Pink)
£34,95 -
Pack 3 Spiky Massage Balls
£20,95 -
Reusable Gel Ice Packs for Shoulder & Back with Compression Band
£20,95 -
Sacroiliac Support Belt (Black)
£24,95 -
Sacroiliac Support Belt (Green)
£24,95 -
Sacroiliac Support Belt (Pink)
£24,95 -
Soft Density Foam Roller for Recovery (Black)
£34,95 -
Soft Density Foam Roller for Recovery (Green)
£34,95 -
Soft Density Foam Roller for Recovery (Pink)
£34,95




























What are the causes and risk factors for hip fractures?
As we highlighted at the beginning of the post, the main cause of hip or femur fractures is osteoporosis, which is normally reported in the elderly.
We list the most relevant factors of all:
- Falls are the most common eventualities that trigger a hip fracture. Either through loss of balance or walking on uneven surfaces, for example.
- Road traffic accidents also cause this type of fracture in people of any age.
- Severe blows or trauma that directly impact the hip are other reasons for this condition.
- Weak bones, due to osteoporosis or other conditions, tend to trigger a bone fracture in this area. Even just by twisting the body while standing.
- In athletes, these fractures may be caused by overexertion.
- In some cases, bone tumours tend to lead to a tear in this category.
- Other common risk factors include chronic medical conditions such as endocrine disorders (e.g. overactive thyroid), brain or nervous system disorders (e.g. dementia, cognitive impairment, Parkinson's disease, stroke, etc.) and intestinal disorders (e.g. those that decrease calcium and vitamin D absorption).
- Poor nutrition or any type of nutritional problem that leads to calcium and vitamin D deficiencies, obesity or low body weight, increases the risk of this bone disease.
- A sedentary lifestyle or physical inactivity tends to weaken bones and muscles, which in many cases is the cause of a hip fracture or a fall that leads to this condition.
- Bad habits, such as excessive alcohol consumption and/or smoking, negatively affect the processes of bone construction and maintenance, leading to a loss of bone mass. This can lead to fractures in the hip and other areas.
- If a person takes medications that contain cortisone or that induce dizziness, drowsiness and weakness, hip fractures can also occur. Since, they are most commonly associated with sudden falls.
- If a person has poor coordination or balance, vision problems, irregular heartbeat or low blood pressure, they are prone to femur or hip fractures.
First aid care to treat a hip fracture
Before seeking medical help, the injured person or those around him or her should take certain first aid measures to prevent the hip fracture from worsening and becoming more serious.
- Immobilising the hip: When these injuries occur, the most important thing is not to move the person until help arrives. Therefore, in this case, it is essential to keep the hip area and its adjacent parts immobile.
- Keep the patient from losing too much heat: To help the patient, the individuals trying to help can wrap or cover the patient in order to prevent the patient's temperature from rising significantly and the loss of body heat.
- Monitor vital signs: As far as possible, it is important to monitor the condition of the person who has suffered the impact. Whether it is taking their pulse, checking that they are breathing normally, or preventing them from closing their eyes and falling asleep. In other words, in short, it is necessary to confirm that they are conscious.
- Medication should not be administered without the approval of professionals: Neither to relieve pain nor to attenuate the different symptoms manifested by the affected person should he/she be medicated with over-the-counter drugs because it may be detrimental to his/her health. Similarly, it is not advisable to give him or her anything to eat or drink.
Most indicated treatments for hip fractures
The most important first aid step for a person who has suffered a hip fracture after diagnosis is to relieve pain. This is usually done by healthcare personnel administering intravenous analgesics and by immobilising the affected limb.
However, fractures of the femur are usually treated with surgical procedures or surgeries aimed at repairing or replacing the broken bone. Since, in most cases, conservative or reserved treatments have unfavourable results and, due to their poor prospects, even tend to increase complications in patients with different conditions.
The operations that are performed to improve a hip fracture are:
- Fixing the fracture using screws: This allows the parts separated by the fracture to be joined together and to simplify their union, sometimes a metal plate is used.
- Installing a metal prosthesis: The aim of this type of surgery is to replace the broken femoral head and/or neck with a prosthesis. This procedure is known as "partial hip replacement".
- Placing a pin into the bone: This offers the possibility of connecting the two portions of the bone that have become dislocated due to the injury. This is usually done when the fracture is low.
- Using a metal prosthesis: Includes the head and neck of the femur along with a new acetabulum. This refers to a total hip replacement which, by default, is used to improve the fracture when the hip is badly damaged, due to chronic osteoarthritis.
Rehabilitation after a hip fracture

Following surgery, a patient with a hip fracture must be treated with anticoagulant drugs. In this way, thrombus formation in the leg veins can be prevented and the risk of developing a pulmonary embolism can be reduced.
In addition, it is essential to start rehabilitation therapy as soon as possible (usually within 24 hours after surgery). During this process, the main focus is on preserving the pre-fracture strength level to maintain mobility and prevent loss of muscle tone. Through this, the patient will be able to regain the ability to walk as he or she did before the bone injury.
In addition, in order to prevent complications such as bedsores from being triggered by lying in the same position, it is recommended that the patient sits on a chair to reduce this risk and even facilitate an upright position. The person should also be encouraged to stand on the healthy leg so that it does not remain stiff and, of course, should do so with the help of another person.
After 4 to 8 days following the operation, rehabilitation exercises should be carried out as long as the patient is able to bear the full weight of his or her body on the injured leg without discomfort or imbalance.
Finally, the affected individual will have to practice different care measures to avoid complications and future injuries for at least one to three consecutive months. These measures should focus on strengthening the muscles of the impacted leg, making allowable efforts and not overstretching their capacity, avoiding certain actions and activities that may re-engage the fractured part of the hip.
Preventive methods to avoid broken hip bones
It is worth noting which are the best ways to avoid or hinder the development of such a bone fracture and here, we specify the most important ones:
- Perform physical activities gradually and consecutively: By nature, exercise is able to increase the amount of bone, tone the muscles and strengthen the joints. This reduces the risk of a fall that can lead to a broken hip bone. When starting this habit, it is essential to do it gradually to avoid overexertion and constantly to get the body used to it.
- Have a healthy and balanced diet: The intake of healthy food is fundamental for the organism to reveal an optimal functioning in general. Taking into account that the proper intake of calcium and vitamin D is vital to maintain bone health, especially throughout adulthood. Therefore, you should consider vitamin supplements rich in these substances and/or eating dairy products and their derivatives, fish, green leafy vegetables, etc.
- Avoid nutritional problems in your body: It is also advisable to do everything possible to avoid low body weight and obesity. These are conditions that increase the risk of suffering a hip fracture.
- Don't practice bad habits such as smoking and drinking alcohol in excess: Since smoking favours the development of osteoporosis, which is one of the main causes of this type of fracture. In addition, alcohol tends to cause bone loss and can cause confusion or disorientation in people (which leads to falls).
- Don't use medication for a long time: In most cases, when an individual is on certain medications for a long time, this tends to reduce the amount of bone in their body and so it is easier for tears to spread. These are usually heparin, corticosteroids and some anti-epileptics.
- Recurrent visits to the doctor: If you suffer from certain pathologies that can promote bone fractures in the hip, it is important to have the appropriate clinical assessment in order to undergo treatment as soon as possible. Whether it is an assessment of mental status, visual assessment and correction, assessment of gait and balance disorders, monitoring and treatment for osteoporosis, etc.
- Do everything possible to prevent falls in your home or workplace: For this, it is usually recommended to practice the following: keeping adequate lighting throughout, removing carpets that move easily, avoiding trip wires, avoiding slippery surfaces (e.g. freshly wet floors, freshly waxed or spilled liquids/food debris), using non-slip mats, installing handrails on both sides of stairs, keeping frequently used items within reach, keeping torches handy in case of a power outage, and leaving furniture in its usual place.
References
- Kannus, P., Parkkari, J., Sievänen, H., Heinonen, A., Vuori, I., & Järvinen, M. (1996). Epidemiology of hip fractures. Bone, 18(1), S57-S63. https://www.sciencedirect.com/science/article/abs/pii/8756328295003819
- Carpintero, P., Caeiro, J. R., Carpintero, R., Morales, A., Silva, S., & Mesa, M. (2014). Complications of hip fractures: A review. World journal of orthopedics, 5(4), 402. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4133447/
- Melton Iii, L. J. (1993). Hip fractures: a worldwide problem today and tomorrow. Bone, 14, 1-8. https://www.sciencedirect.com/science/article/abs/pii/8756328293903417
- Cooper, C., Campion, G., & Melton, L. 3. (1992). Hip fractures in the elderly: a world-wide projection. Osteoporosis international, 2, 285-289. https://link.springer.com/article/10.1007/BF01623184
- Cummings, S. R., & Nevitt, M. C. (1989). A hypothesis: the causes of hip fractures. Journal of gerontology, 44(5), M107-M111. https://academic.oup.com/geronj/article-abstract/44/5/M107/696714
- Müller, M. E., Nazarian, S., Koch, P., & Schatzker, J. (2012). The comprehensive classification of fractures of long bones. Springer Science & Business Media. https://books.google.es/books?hl=en&lr=&id=t0CgBQAAQBAJ
- Watson-Jones, R. (1962). Fractures and joint injuries. E. & S. Livingstone. http://117.239.25.194:7000/jspui/bitstream/123456789/1853/7/INDEX.pdf
- Hoppenfeld, S., & Murthy, V. L. (Eds.). (2000). Treatment and rehabilitation of fractures. Lippincott Williams & Wilkins. https://books.google.com/books?hl=en&lr=&id=bxhycwgJUtQC
- Kanis, J. A., Borgstrom, F., De Laet, C., Johansson, H., Johnell, O., Jonsson, B., … & Khaltaev, N. (2005). Assessment of fracture risk. Osteoporosis international, 16, 581-589. https://link.springer.com/article/10.1007/s00198-004-1780-5
- BAILEY, M. (1982). Emergency! First aid for fractures. Nursing2021, 12(11), 72-81. https://journals.lww.com/nursing/Citation/1982/11000/EMERGENCY__FIRST_AID_FOR_FRACTURES.22.aspx