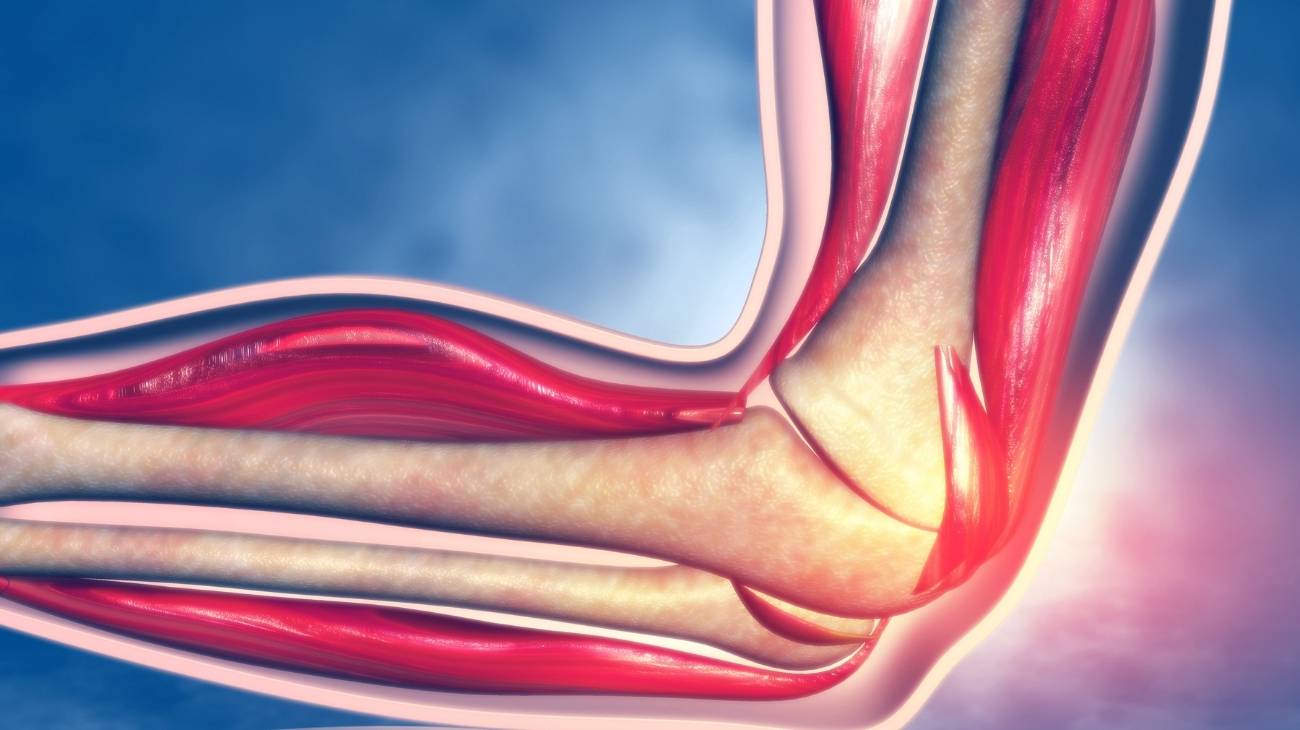
Knee Anatomy
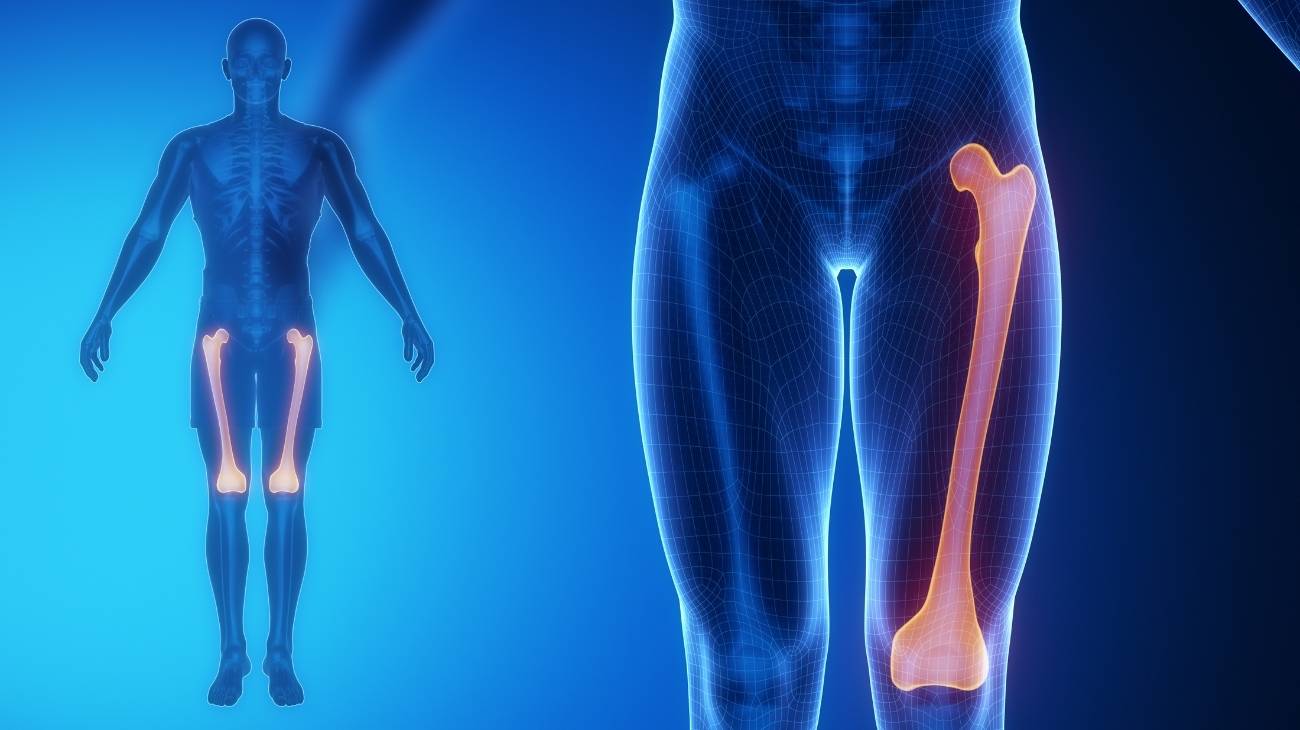
The knee is a joint located in the middle of the leg. It allows the femur to join the tibia, which helps to perform flexion and extension movements. These actions result in the patellar area being one of the most injury prone.
Featured Categories