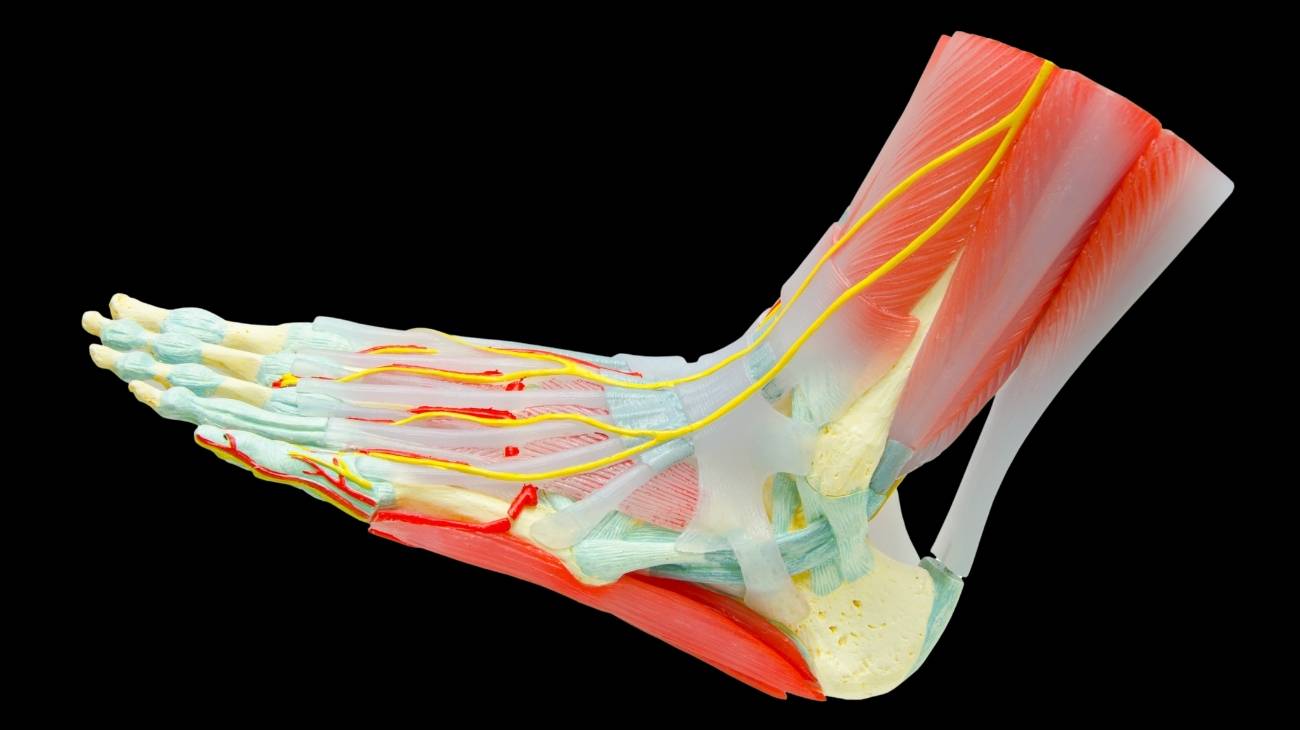
Foot Anatomy
The bones, muscles and ligaments of the foot are an important part of the anatomy of this joint body. For this reason, it is convenient to develop them so that you know in depth their location and their functioning. This will help you to know in a preventive way and to avoid foot contusions.
Featured Categories