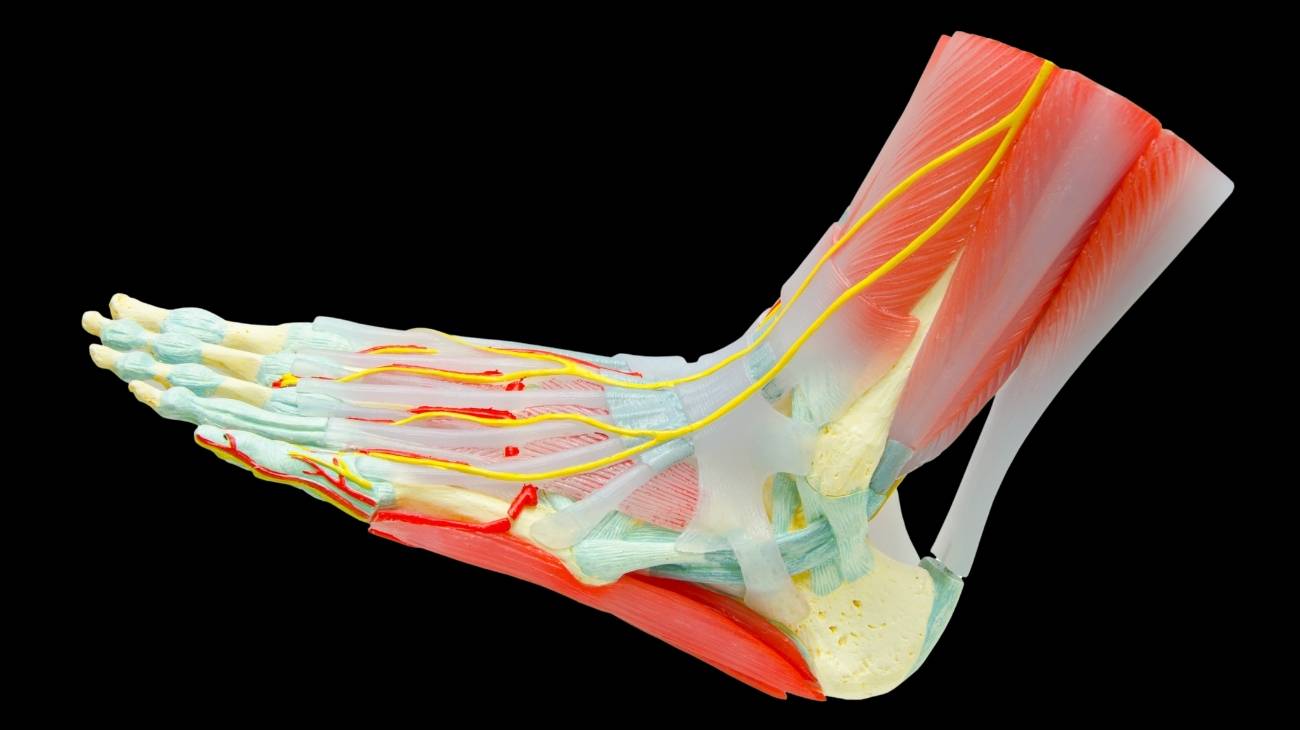
The bones, muscles and ligaments of the foot are an important part of the anatomy of this joint body. For this reason, it is convenient to develop them so that you know in depth their location and their functioning. This will help you to know in a preventive way and to avoid foot contusions.
If you want to know which are the most common injuries that occur in this part of the body, you need to continue reading. We will explain, in detail, the biomechanics of the foot and the treatments that can be applied to improve the pain.
Parts and anatomy of the foot
Bones and joints
The bony anatomy of the foot is made up of the following bones, listed from proximal to distal
- Calcaneus: One of the strongest bones in the human body, it forms the person's heel. It is located below the scaphoid and talus, so it also connects to the wedges and cuboid.
- Astragalus: This bony tissue is what gives rise to the foot and connects to the tibia and fibula of the leg. It can be found above the calcaneus to cause joint movement.
- Scaphoid or navicular: This bone is found on the top of the foot, above the cuboid. It also joins with the talus and the three wedges.
- Cuboid: This is one of the bones responsible for giving balance and support to the foot. It connects to the calcaneus, the talus, below the scaphoid and to the lateral cuneiform.
- Lateral wedge or cuneiform: This bone allows articulation of the third metatarsal and is connected to the medial wedge, navicular and cuboid.
- Intermediate wedge: This bone can be found at the top of the instep and its function is to join the scaphoid to the second metatarsal. It is located between the internal and lateral wedge.
- Medial cuneiform or internal wedge: This bone is located at the back of the foot and is responsible for the articulation of the foot. It connects to the medial cuneiform and the first metatarsal.
- Metatarsals: In this group of bones they can be divided from the first to the fifth metatarsal, the first metatarsal being considered the internal bone that is connected to the proximal phalanx of the big toe and the internal cuneiform.
- Phalanges: These bones are divided into three sections, called distal, medial and proximal. The distal phalanx is attached to the metatarsal. Like the hand, the great toe does not have a medial phalanx.
As for the joints that allow the movements proper to the human foot to be given, the following can be mentioned:
- Anterior medial subtalar: A joint necessary for the accommodation of the foot, connecting the talus - from the inner facet - with different ligaments. It is part of the astragalotarsal group of joints.
- Posteroexternal subtalar: It has the same function as the previous joint, but its origin is in the upper astragalar part.
- Chopart: Named after the discoverer and scholar of this joint. It joins the calcaneus and the posterior facet of the cuboid. The calcaneocuboid is a triangular joint that allows autonomous movements between the two bones.
- Astragalo-scaphoid: The scaphoid and talus join at this joint to give movement to the back of the foot.
- Astragalocalcaneo-scaphoid: A joint that makes small movements between the scaphoid, calcaneus and talus. It is included in the astragalotarsal joint group.
- Cuneonavicular: The three wedges articulate with the anterior area of the scaphoid through this articular body.
- Cubo-cuneus: This is another joint located between the anterior tarsal bones. The fourth and fifth toes join with the internal wedge and the posterior part of the cuboid.
- Intercuneiform: These joints also belong to the anterior tarsal area and are responsible for moving the three cuneiforms or wedges.
- Lisfranc or tarsometatarsal joint: The five metatarsals can articulate with the nails and the cuboid through this joint.
- Metatarsophalangeal joints: The metatarsal joint is the joint between the metatarsals and the phalanges, which causes the toes to move. They are also known as interphalangeal joints.
- Supra-astragalar: It can be considered part of the ankle or the foot. It is responsible for carrying out the movements in the form of a pulley so that this area of the foot can carry out extension and flexion actions. It joins the tibia to the talus.

Muscles
The muscles found in the foot are:
- Extensor hallucis brevis: This muscle allows the toe to contract to produce the extension movement. It arises from the calcaneal bone and inserts into the proximal phalanx of the big toe.
- Extensor digitorum brevis: As in the previous muscle, this tissue allows the extension of the rest of the toes. It ends at each of the proximal phalanges of the toes and extends from the calcaneus.
- Flexor hallucis brevis: Located in the deep plane, this intrinsic muscle develops on the inside of the foot from the cuboid to the phalanx of the hallux (or big toe). It allows flexion movement.
- Flexor digitorum brevis of the fifth toe: This muscle runs from the fifth metatarsal to the first phalanx of the fifth toe. It can be seen on the top and outside of the foot.
- Opponent of the fifth toe: This is a muscle that allows flexion and approximation movements of the little toe in relation to a plantar and medial view. It develops from the plantar aponeurosis to the three phalanges of the toe mentioned.
- Adductor hallucis: On the top of the foot, the development of this V-shaped muscle can be seen. It runs from the plantar aspect of the cuboid bone, the medial cuneiform to the area of the second to fourth metatarsal. On the other hand, its origin also occurs at each of the metatarsophalangeal joints of the third to fifth toes. It inserts into the first phalanx of the big toe. Its mission is to cause adduction of the big toe.
- Abductor hallucis: Abduction and flexion of the big toe is achieved by the action of this muscle. It is located on the superficial part of the foot and runs from the calcaneus to the first phalanx of the big toe.
- Little toe abductor: As in the previous muscle, it also balances the longitudinal arch of the foot. It originates from the plantar fascia and inserts on the proximal phalanx of the fifth toe.
- Flexor digitorum brevis: It arises from the internal tubercle of the calcaneus, in the plantar fascia, and extends to the second phalanx of the second to fifth toes by means of a tendon. Flexion of the aforementioned phalanges is the main work of this muscle.
- Lumbrical: This is a set of four muscles that allow flexion of the metatarsophalangeals of the second to fifth toes. It arises from the tendons that originate from the flexor digitorum longus, in its medial part, and inserts in the proximal phalanges.
- Accessory flexor digitorum: Also known as plantar quadratus, it is a muscle that works in flexion of the second to fifth toes inclusive. It travels from the calcaneus to the tendon of each toe via the flexor muscle.
So far we have developed the intrinsic muscles of the foot, but these are not the only ones, as this joint is related to the leg. For this reason, it is useful to name the following tissues that pass from the leg to the foot and can be part of both areas.
These are:
- Soleus: Together with the calf muscles, they form the triceps suralis. Plantar flexion is carried out thanks to the action of this muscle which originates in the fibula and tibia.
- Gastrocnemius or calf muscle: Its different portions allow flexion of the foot. It originates in the condyle of the femur and develops to the calcaneus under the name of the Achilles tendon.
- Flexor hallucis longus: It arises from the fibula and attaches to the distal phalanx of the big toe. Thanks to this muscle, flexion of the big toe is possible.
- Flexor hallucis longus: The remaining toes also have a muscle that allows flexion. Its course is produced in the tibia, in its posterior facet, and ends in the last phalanx of each of the toes.
- Posterior tibialis: This elongated muscle arises from the tibia and fibula and inserts into the medial cuneiform bone, the navicular bone and the metatarsals. Its work consists of adduction and flexion of the sole of the foot.
- Tibialis anterior: From the lateral surface of the tibia to the first metatarsal and the medial cuneiform, the path of this muscle can be seen. Thanks to its action, it allows inversion and flexion.
- Extensor hallucis longus: The interosseous membrane and the medial surface of the fibula give rise to this muscle which inserts into the distal phalanx of the hallux.
- Extensor digitorum longus: The 2nd to 5th toes can be extended by this muscle, which originates from the tibia and fibula. It attaches to the phalanges of each of the digits by means of tendons.
- Peroneus longus lateralis: It is a muscle that allows eversion of the foot. It runs from the head and tuberosity of the fibula to the first metatarsal.
- Peroneus lateralis brevis: Like the previous muscle, it arises from the fibula and develops on the outside of the leg until it inserts on the fifth metatarsal. Its action allows different biomechanical movements, the most important being eversion and plantar flexion.
- Third peroneus: This muscle allows dorsal flexion and eversion. It is located on the outside of the leg, arising from the fibula and inserting on the fifth metatarsal. It is also known as the anterior peroneus.

Ligaments
The ligaments that make up the anatomy of the foot are
- Anterior and posterior tibiotalar: These ligaments are triangular in shape and serve to join the talus with the tibial malleolus from the posterior or anterior tubercle, hence their name.
- Tibiocalcaneal: This is a ligament that arises from the malleolus of the tibia, just on the anterior tubercle. It inserts on the medial side of the calcaneal process, which allows plantar movements of the foot.
- Tibionavicular: It allows the union of the tibia, through its malleolus, with the navicular bone in its dorsal part.
- Tibio-scaphoid: At the tubercle of the malleolus of the tibia it begins its course to the medial surface of the scaphoid bone. This allows plantar flexion.
- Dorsal astragalonavicular: The navicular with the talus connect in the dorsal part of the foot through this tissue. It is also known as the talonavicular ligament.
- Dorsal and plantar cuneonavicular: Ligaments located from the tibialis posterior to the dorsal or plantar part of the navicular bone.
- Dorsal intercuneiform: These ligaments are divided into three bands, which join the second, third and fourth parts of the cuneiform with the cuboid bone.
- Dorsal tarsometatarsal: A group of ligaments located in the dorsal part of the foot that join the first cuneiform to the first metatarsal. Another connects the three cuneiforms to the first metatarsal, another connects the third cuneiform to the metatarsal, and another connects the cuboid to the third cuneiform. The last ligament joins the cuboid to the first metatarsal.
- External calcaneoastotalar: The calcaneus and talus bones are joined by this ligament from the outside of the foot. This group of ligaments is also known as the talocalcaneal ligament.
- Inner calcaneoastotalar: The grooves of both bones see the path of this ligament necessary for foot flexion.
- Posterior calcaneoastotalar: The posterior aspects of the talus and calcaneus give rise to and insert the ligament belonging to the articular body.
- Interosseous calcaneoastotalar: joins the calcaneus to the talus on the superior and inferior surfaces, respectively.
- Short plantar: It runs from the cuboid to the calcaneal bone, which allows movements to be made in the lower plantar area of the foot.
- Plantar long: Unlike the short plantar ligament, this tissue develops from the peroneus lateralis longus to the first metatarsal, and its action in the plantar arch is very important.
- Plantar calcaneonavicular: This ligament is located on the lower part of the foot, joining the calcaneus sustentaculum with the posterior area of the navicular.
- Calcaneocuboid: This ligament is found on the outside of the foot and is designed to join the cuboid to the calcaneus, which allows for movement of the ankle. It can be divided into dorsal and plantar, according to the location of the insertion on the cuboid.
- Cuneocuboid: Can be divided into dorsal and plantar. It develops from the third cuneiform to the cuboid, in its dorsal or plantar part (from this derives its classification).
- Dorsal cuboidonavicular: This is a ligament located obliquely between the scaphoid and the cuboid.
- Anterior and posterior talofibular: Located in both areas of the ankle, these ligaments join the talus, calcaneus and fibula. Their function is to support the joint so that the foot can perform extension and flexion movements.
- Calcaneofibular: It has a non-isometric function when the foot is in plantar or dorsal flexion. It is located on the outside of the foot between the talus, navicular and cuboid.
- Tibiofibular: This ligament can be divided into two sections, anterior and posterior. It originates at the anterior lateral (or posterior) end of the tibia to the fibular tubercle. This allows axial movements of the ankle.

Best products for foot and leg pain relief
Bestseller
-

2 Ankle Compression Sleeve (Black/Gray)
$19.95 -
2 Ankle Compression Sleeve (Green/Navy)
$19.95 -
2 Ankle Compression Sleeve (Pink/Bordeaux)
$19.95 -
Acupressure Mat and Pillow (Black/Gray)
$49.95 -
Acupressure Mat and Pillow (Green/Navy)
$49.95 -
Acupressure Mat and Pillow (Pink/Bordeaux)
$49.95 -
Acupressure Pillow (Black/Gray)
$29.46 -
Acupressure Pillow (Green/Navy)
$29.46 -
Acupressure Pillow (Pink/Bordeaux)
$29.46 -
Electric Foot Massager
$58.97 -

Foot Massage Roller for Plantar Fasciitis (Black)
$19.95 -
Foot Massage Roller for Plantar Fasciitis (Green)
$19.95 -
Foot Massage Roller for Plantar Fasciitis (Pink)
$19.95 -
High Density Foam Roller for Muscle (Black/Gray)
$24.95 -
High Density Foam Roller for Muscle (Green/Navy)
$24.95 -
High Density Foam Roller for Muscle (Pink/Bordeaux)
$24.95 -
Ice Massage Roller Ball (Black)
$39.95 -
Ice Massage Roller Ball (Green)
$39.95 -
Ice Massage Roller Ball (Pink)
$39.95 -
Ice Pack for Foot - Cold Therapy Socks (Black)
$24.95 -
Ice Pack for Foot - Cold Therapy Socks (Green)
$24.95 -
Ice Pack for Foot - Cold Therapy Socks (Pink)
$24.95 -
Microwavable Heated Slippers (Hearts)
$24.95 -
Microwavable Heated Slippers (Oxford)
$24.95 -
Microwavable Heated Slippers (Sport)
$24.95 -
Microwaveable Heating Pad for Pain Relief (Hearts)
$19.95 -
Microwaveable Heating Pad for Pain Relief (Oxford)
$19.95 -
Microwaveable Heating Pad for Pain Relief (Sport)
$19.95 -
Pack 2 In 1 Foam Roller High + Soft Density (Black/Gray)
$29.95 -
Pack 2 In 1 Foam Roller High + Soft Density (Green/Navy)
$29.95 -
Pack 2 In 1 Foam Roller High + Soft Density (Pink/Bordeaux)
$29.95 -
Pack 3 Spiky Massage Balls
$19.95 -
Pack Lacrosse Massage Balls & Peanut Roller
$29.95 -
Reusable Gel Ice Packs for Ankle & Foot with Compression Band
$19.95 -
Reusable Gel Ice Packs with Compression Band for Sports Injury
$19.95 -
Soft Density Foam Roller for Recovery (Black)
$24.95 -
Soft Density Foam Roller for Recovery (Green)
$24.95 -
Soft Density Foam Roller for Recovery (Pink)
$24.95 -
Sport Compression Socks (1 Pair) (Black/Gray)
$19.95 -
Sport Compression Socks (1 Pair) (Green/Navy)
$19.95 -
Sport Compression Socks (1 Pair) (Pink/Bordeaux)
$19.95 -
Vibrating Foam Roller
$35.36 -
Vibrating Massager Ball
$35.36















































Biomechanics of the foot
The biomechanical movements that occur in the foot are
- Adduction: This consists of lifting the toe of the foot towards the anterior part of the tibia. It can be combined with supination and pronation movements thanks to the anterior internal subtalar joint. It can be opened up to 30°.
- Abduction: It is the opposite movement to the adoption, so it is developed when it is placed on the distal part of the foot downwards. It can also be combined with pronation and supination work.
- Dorsal flexion: This biomechanical action is performed by the movement of the tibia when the foot is supported to the anterior aspect of that bone. Its maximum amplitude is 20° due to the toe extensors and plantar flexors.
- Plantar flexion: This movement is called in biomechanics when the foot is placed as far as possible, at a maximum of 45°, in relation to the leg.
- Eversion: This is a characteristic movement of the foot which consists of raising the lateral part of the foot towards the external part of the same leg. This causes the sole of the foot to move a maximum of 25° outwards from the body.
- Inversion: This is the opposite action to eversion, as it consists of bringing the sole of the foot up to 35° towards the inside of the body. In this way the sole can touch the ankle of the other leg thanks to the peroneals and flexors.
- Supination: This is a movement that consists of a combination of inversion, plantar flexion and abduction. With this action it is possible to place the sole of the foot on the inside of the body. The subtalar joint and the tibial muscles are involved in this movement.
- Pronation: This is the opposite of supination and also consists of combining the biomechanical movements of eversion, abduction and dorsiflexion. This can be done thanks to the Lisfranc joint and the peroneal and tibial muscles.
Most common foot injuries
Among the most common foot injuries we can divide them into two groups, which are:
Types of foot injuries
The types of ailments that can be generated in the feet according to their origin in previous diseases are the following:
- Osteoarthritis of the feet: This chronic disease can occur anywhere in the foot, but the most common areas are the ankle joint body, the medial area (medial talar osteoarthritis) and the big toe. This is wear and tear on the cartilage and bones in the joint areas of the foot.
- Achilles tendon bursitis: Achilles bursitis is inflammation that occurs in the synovial sac located in the back joint of the ankle. This is due to excess joint fluid in the bursa, causing pain and immobility of the foot.
- Muscle cramps in the feet and toes: The causes that can lead to this ailment can be varied, but the most common are a lack of magnesium and potassium, dehydration, inadequate footwear and the patient's age. The deep tingling sensation usually appears in the big toe and metatarsal area.
- Sprained foot: This is an ailment caused by the rupture or excessive stretching of a ligament in the foot. Any of its 3 degrees can arise for different reasons, the most common being excessive activity or a sedentary lifestyle. This causes pain, inflammation and joint stiffness.
- Fractures in the foot: The most common fractures that occur in the foot are those that occur in the metatarsals and phalanges. These injuries can be caused by trauma, blows or falls. It is necessary to use compressive clothing to cure this condition.
- Plantar fasciitis: The plantar fascia is a tissue located on the bottom of the foot, which connects the calcaneal bone to the toes, helping to create the plantar arch. When this tissue becomes inflamed, it causes a shooting pain near the calcaneus (heel), especially after a night's rest.
- Achilles tendon tendonitis: When there is inflammation or involuntary contracture of the Achilles tendon, the person feels pain when walking, numbness and warmth in the back of the foot. This can be caused by excessive activity, poor posture for tasks and poor blood supply.
Sports injuries to the feet
Athletes playing these sports are prone to injure different parts of the foot. Take a look:
- Foot, ankle and leg injuries in basketball: The demanding activity produced by this sport can lead to plantar fasciitis, Achilles tendonitis, Achilles tendon bursitis, sprains in the deltoid and calcaneofibular ligaments breaks in the calcaneus and metatarsals.
- Foot injuries in soccer: Sprains of the posterior and anterior peroneoastotalar tendon are the most frequent injuries suffered by people who play soccer. However, it is also possible to find tendinopathies, inflammation in the bursae of the Achilles tendon and dorsal ruptures of the foot.
- Foot and ankle injuries in gymnastics: Plantar fasciitis; tibioperoneal, peroneoastragal and deltoid sprains; muscle contractures; dislocations and fractures of the calcaneus, talus, tibia and fibula are the most common sports injuries to the feet.
- Running injuries to the foot: This activity causes injuries to the plantar fascia, inflammation of the intercuneiform and tibionavicular ligaments, ankle sprains and calcaneal and toe fractures. Osteoarthritis of the big toe and ankle joint can also occur.
- Ankle and foot injuries in tennis: Calcaneoperoneus, peroneoastotalar and deltoid sprains are the most frequent ailments that tennis players have in this part of the body. There are also athletes with dislocations and muscle contractures of the foot, achilles bursitis and tendinopathies. Tennis toe or jogger's toe is characteristic of this sport.
Foot diseases and ailments

In addition to the foot injuries mentioned above, it is also possible to find these diseases and ailments in this area of the body:
Gout
Excess uric acid that is not eliminated by the blood causes inflammation, redness and stiffness in the big toe, although it can also affect the heel and ankle. This disease can also be caused by arthritis.
Thickening of the skin
Due to constant activity and friction between this tissue and the footwear, calluses may appear on the distal part of the foot, usually on the lateral and upper area. It is also common to find people with calluses on the heels.
Hammertoes
This abnormality occurs in the foot when there is an imbalance between the ligaments of the tensor muscles of the phalanges causing constant bending of the toes. This causes pain, redness and contracture in the big toe.
Bacteria and nail fungus
Many people remove the cuticle of the toenails for beauty reasons. This action puts the immune system of the nails at risk, as the protective barrier against fungi and bacteria is removed. Among the most well-known conditions is ringworm of the foot or athlete's foot. It is possible that these micro-organisms appear due to trauma and previous injuries.
Falling of the arch of the foot
This is also known as flat feet. This is a decrease in the attention of the plantar fascia tissues, which can lead to malfunction in the ankle and foot joint, causing - in some cases - pain and swelling.
Metatarsalgia
This discomfort occurs on the sole of the foot, under the toes and at the junction between the metatarsals and the first phalanges. It is an inflammation that is generated by the excessive and demanding activity practised by the patient.
Plantar fibromatosis
Also known as Ledderhose disease, which is a condition that occurs in the plantar aponeurosis with the appearance of nodules or proliferative tissues. Pain appears in more advanced stages of this condition.
Macerated dermatitis
This is one of the most common diseases that people suffer from on their feet. Its main symptom is a bad smell caused by a fungus that appears due to excessive sweating and lack of ventilation in the foot.
How can we relieve foot and leg pain through complementary and non-invasive therapies?
Complementary and non-invasive therapies used to treat foot ailments and diseases are as follows
Heat and cold therapy
Through the application of specific products, such as heat packs with hot and cold gel or microwavable heat packs, it is possible to stimulate the area to reduce inflammation and benefit blood flow. This will improve the elimination of toxic substances in the tissues, causing the ailment to go into remission faster. Its practice must be monitored by a doctor, as each session cannot exceed 5 minutes at each temperature.
Compression therapy
Compression garments are a very efficient alternative and non-invasive therapy to help keep the affected area immobile and to put pressure on the capillary walls to improve the exchange of nutrients with the blood. Compression socks and stockings, compression sleeves and ankle braces are commonly used for this purpose. Elastic bandages are also available for sports.
Massage therapy
Massage is a very effective treatment to reduce involuntary tensions in muscles and tendons. For this, it is necessary to use a professional therapist to apply the rubbing correctly. In some cases it is possible to perform self-massage by means of electric foot massagers, such as rollers, cushions and massage guns.
Acupressure therapy
This oriental technique helps to stimulate the nervous system and blood flow to reduce inflammation and foot pain. Acupressure mats, cushions, massage balls and massage hooks can be used for this. It is also possible to do this practice with a professional, so it is always advisable to consult a doctor before choosing this non-invasive therapy.
Thermotherapy
One of the most important benefits of heat is to reduce stress in the affected area by dilating the blood vessels. This helps to improve the gas exchange between the blood and the tissues and quickly brings about a feeling of well-being. Different techniques can be applied, but the most recommended non-invasive treatments for these cases are the use of thermal pillows for microwaves, packs with gels or foot baths (footbaths).
Cryotherapy
Reducing inflammation in the feet by means of cold is a good option as long as you have consulted your doctor beforehand. It can be applied by immersion in cold capsules or by choosing manual products that generate this temperature in a controlled manner. The latter include packs with cold gels or thermal pillows for hot and cold.
Electrical muscle stimulation (EMS)
Muscle electrostimulation, or EMS, is a therapy that consists of stimulating muscle contractions through the use of electricity, so as to achieve an effect of activity and hypertrophy as in the gym, but without the need to go to any sports center. This means that you can put your muscles to work without leaving home.
Electrotherapy
This is a technique that seeks relief from pain and some physical ailments through the application of electrical and electromagnetic energy, among other variants, through the skin with the use of conductive pads called electrodes. It is a very safe type of therapy and must be applied by a physical therapist specialized in the manipulation of electricity to treat some kinds of ailments.
Myofascial release therapy
Also known as myofascial induction, this therapy consists of the application of manual massage to treat the shortening and tension generated in the myofascial tissue that connects the muscles to the bones and nerves. For this purpose, various massage techniques are used that focus on the so-called trigger points.
Percussion Massage Therapy
Vibration or percussion massages are precise, rhythmic and energetic strokes on the body to achieve relief from some annoying symptoms when muscle fibers are tightened, often by a high workload on them and that has left trigger points in the muscle fibers.
R.I.C.E Therapy
The R.I.C.E. therapy is the first and simplest of the treatment protocols for minor injuries. It appears in the sports field to deal with accidents involving acute injuries. For many years, it has been considered the most suitable for its speed and results.
Trigger points therapy
Myofascial pain points or trigger points are knots that are created in the deeper muscle tissues, causing intense pain. The pain does not always manifest itself right in the area where the point develops, but rather this pain is referred to nearby areas that seemingly do not appear to be related. In fact, it is estimated that more than 80% of the pain they cause manifests in other parts of the body.
Other effective alternative therapies
On the other hand, it is also possible to find the following effective alternative therapies to treat foot complaints:
- Natural remedies using plants: Footbaths help to reduce pain, swelling and redness of the feet. For this it is necessary to apply a warm water bath with natural herbs and plants that contain anti-inflammatory components. Among the most common are ginger, mint and lavender.
- Acupuncture: This therapy aims to focus on the patient's mind to cope with foot pain. This is applied when the condition is advanced, as it manages to reduce stress and find an emotional balance in the person through the use of special needles.
- Kinesiotherapy: Before choosing this complementary treatment, it is necessary to consult a doctor to assess whether the movements and exercises carried out in the therapy are suitable for the condition to go into remission. If so, the person should perform targeted actions that stimulate the development of the joint area.
- Aromatherapy: This is one of the therapies that seeks to reduce the patient's stress through relaxation. To reach this stage, the person must naturally inhale different aromas that help to find psychological harmony. Mint, lemon, orange and some essential oils are products used in this treatment.
References
- Dawe, E. J., & Davis, J. (2011). (vi) Anatomy and biomechanics of the foot and ankle. Orthopaedics and Trauma, 25(4), 279-286. https://www.sciencedirect.com/science/article/abs/pii/S1877132711000303
- Kelikian, A. S., & Sarrafian, S. K. (Eds.). (2011). Sarrafian's anatomy of the foot and ankle: descriptive, topographic, functional. Lippincott Williams & Wilkins. https://books.google.es/books?hl=en&lr=&id=I8h6bDR0SLMC
- Abboud, R. J. (2002). (i) Relevant foot biomechanics. Current Orthopaedics, 16(3), 165-179. https://www.orthopaedicsandtraumajournal.co.uk/article/S0268-0890(02)90268-9/fulltext
- Chan, C. W., & Rudins, A. (1994, May). Foot biomechanics during walking and running. In Mayo Clinic Proceedings (Vol. 69, No. 5, pp. 448-461). Elsevier. https://www.sciencedirect.com/science/article/abs/pii/S0025619612616425
- Chinn, L., & Hertel, J. (2010). Rehabilitation of ankle and foot injuries in athletes. Clinics in sports medicine, 29(1), 157-167. https://www.sportsmed.theclinics.com/article/S0278-5919(09)00071-4/fulltext
- Subotnick, S. I. (1985). The biomechanics of running implications for the prevention of foot injuries. Sports Medicine, 2(2), 144-153. https://link.springer.com/article/10.2165/00007256-198502020-00006
- Haapamaki, V. V., Kiuru, M. J., & Koskinen, S. K. (2004). Ankle and foot injuries: analysis of MDCT findings. American Journal of Roentgenology, 183(3), 615-622. https://www.ajronline.org/doi/full/10.2214/ajr.183.3.1830615
- Riskowski, J. L., Hagedorn, T. J., & Hannan, M. T. (2011). Measures of foot function, foot health, and foot pain. Arthritis care & research, 63(0 11), S229. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4155931/
- Leveille, S. G., Guralnik, J. M., Ferrucci, L., Hirsch, R., Simonsick, E., & Hochberg, M. C. (1998). Foot pain and disability in older women. American journal of epidemiology, 148(7), 657-665. https://academic.oup.com/aje/article/148/7/657/148386
- Benvenuti, F., Ferrucci, L., Guralnik, J. M., Gangemi, S., & Baroni, A. (1995). Foot pain and disability in older persons: an epidemiologic survey. Journal of the American Geriatrics Society, 43(5), 479-484. https://agsjournals.onlinelibrary.wiley.com/doi/abs/10.1111/j.1532-5415.1995.tb06092.x